



At Dermatology Associates of Ithaca, we offer world class skin cancer diagnosis and treatment for our patients. Although a diagnosis of skin cancer can be disheartening, we stand ready to guide our patients through the diagnosis and treatment process with compassion and expertise:
Clinical Diagnosis – Our providers are expertly trained in the early detection of skin cancer, which can be found via a complete skin examination. To learn more about skin cancer prevention, please click here for our Skin Cancer Prevention handout.
Skin Biopsies – Skin biopsies are performed on any suspicious lesions after numbing medicine has been applied, to minimize patient discomfort. Biopsy specimens are sent to our world class dermatopathology laboratory where fellowship-trained dermatopathologists analyze the specimen under the microscope and generate a detailed report communicating their findings. If you’ve had a skin biopsy procedure at our office, you can find skin biopsy care instructions here.
Pathology Report Interpretation – Dr. McAllister interprets the pathology reports and creates treatment plans specific for each patient, to maximize cure in a minimally invasive way. Dr. McAllister and her team have decades of experience in detecting and treating skin cancer, particularly basal cell carcinoma, squamous cell carcinoma, and melanoma. To learn more about quality and collaboration in dermatopathology, please click here .
Discussion of Results – All patients who have had a biopsy should call in two weeks to check on their results. If further treatment is needed, we will fully explain the results of the biopsy and treatment plan.
Treatment Options – We offer a number of different skin cancer treatments, tailored to the type of skin cancer, the location on the body, and other variables depending on the individual patient’s needs. Our office performs surgical excisions, electrodessication and curettage, and other treatments according to each patient’s medical condition.
Excisional Surgery – We offer patients in Ithaca and the surrounding areas surgical excision in our offices to treat both benign and cancerous lesions. We recommend surgical excision when clear margins are needed to prevent recurrence and spread of the lesion.
Mohs Surgery – During Mohs surgery, thin layers of cancer-containing skin are progressively removed and examined until only cancer-free tissue remains. Mohs surgery is also known as Mohs micrographic surgery.
Skin Cancer Prevention – Sun protection is essential to skin cancer prevention – about 90% of non melanoma skin cancers and about 86% of melanomas are associated with exposure to UV radiation from the sun.
Skin Cancer
Skin cancer results from the unregulated proliferation of abnormal skin cells. It is triggered when unrepaired DNA damage to skin cells (most often due to ultraviolet radiation from the sun or from tanning beds) causes mutations that allow the skin cells to grow uncontrollably and to create malignant tumors.
Basal Cell Carcinoma (BCC)
BCC is the most common type of skin cancer, with more than 2,000,000 cases diagnosed in the United States every year. BCC rarely spreads beyond the original tumor site, but can grow wide and deep, invading into tissue and bone if left untreated. BCC’s can look like non-healing open sores, bright pink patches, acne bumps that do not resolve within a couple of months, or shiny bumps with blood vessels. Fortunately, this type of skin cancer generally grows very slowly and rarely spreads to other organ systems. Basal cell carcinoma can have a variety of appearances ranging from clear bumps with prominent blood vessels to chronic non-healing wounds.
Squamous Cell Carcinoma (SCC)
SCC is the second most common type of skin cancer with approximately 700,000 cases in the U.S. per year. If detected early, SCC can be easily removed and treated; however, if allowed to grow, approximately 2% of SCCs can penetrate other organ systems and cause disfigurement and death (depending on different estimates, as many as 8,800 people die from the disease every year). SCC is primarily caused by cumulative ultraviolet (UV) exposure over the course of a lifetime, including daily exposure to the sun, intense exposure to the sun during the summer months, and direct exposure to UV radiation via tanning beds. Squamous cell carcinoma presents as bright pink patches, open sores, elevated growths with an overlying horn, or warty growths, often with crusting and bleeding.
Treatment of BCC and SCC
After the diagnosis is made via skin biopsy, the choice of treatment depends on the tumor’s type, size, and location. Most of the time, treatment can be performed on an outpatient basis in our office. A local anesthetic is used during most surgical procedures to minimize discomfort. Basal cell and squamous cell skin cancer treatment is often accomplished with surgical excision, which offers results that are both medically and cosmetically excellent.
Alternatively, if the borders of the skin cancer are difficult to define, or if the skin cancer has complex features or is located in an area where tissue preservation is critical, Mohs surgery may be recommended. Treatment with surgical excision or Mohs surgery often (but not always) requires placing sutures (stitches) to close up the wound after surgery patients. Until the sutures are removed in one to two weeks after surgery, patients should avoid vigorous exercise or stretching of the treated areas. Scars are usually small and improve with time.
Other treatments such as electrodessication and curettage, which has a lower cure rate and leaves a hypopigmented round scar, or Aldara or Efudex cream which also have a lower cure rate and may result in severe irritation and redness during the course of treatment, may be considered based on individual patient and tumor factors. Once a patient has been diagnosed with BCC or SCC, they are at risk for recurrence and the development of new skin cancers, so we recommend close monitoring on a semi-annual or annual basis via full skin exams in our office.
Melanoma
The deadliest type of skin cancer, melanoma is less common than BCC or SCC, with approximately 100,000 cases per year in the United States. If recognized and treated early, melanoma is almost always curable. However, when not detected early enough melanoma can spread quickly to other parts of the body and be deadly. Melanoma kills over 10,000 people per year in the United States. Melanomas often resemble moles, with some developing from moles. They are usually black or brown, but can also be skin-colored, pink, red, purple, blue, or white. Since early detection is crucial, patients with a personal or family history of melanoma, and those with other risk factors for melanoma (e.g. history of blistering sunburns, extensive sun or tanning bed exposure, history of radiation therapy, history of immunosuppression, etc.) are encouraged to undergo regular skin surveillance with a dermatologist.
Treatment of Melanoma
Once a melanoma is diagnosed, Dr. McAllister interprets the pathology report to determine the best and safest treatment course. For low risk lesions, a surgical excision is performed at Dermatology Associates of Ithaca with standard recommended safety margins to maximize the possibility of cure. Cure rates for melanoma detected in the early stages, particularly in patients who return for regular full skin exams, can exceed 95%. For higher risk lesions, we also collaborate with our colleagues in plastic surgery and surgical oncology to perform a wide local excision with an additional procedure called a sentinel node biopsy which can determine whether the melanoma has spread and whether further treatment is necessary.
The Warning Signs
A skin growth that increases in size and appears pearly, translucent, tan, brown, black, or multicolored.
A mole, birthmark, beauty mark, or any brown spot that:
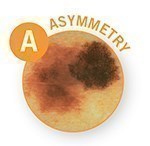 A = Asymmetry
A = Asymmetry
One half is unlike the other half.
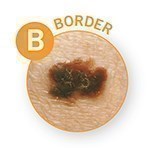 B = Border
B = Border
An irregular, scalloped or poorly defined border.
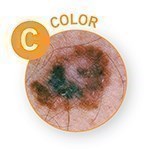 C = Color
C = Color
Is varied from one area to another; has shades of tan, brown or black, or is sometimes white, red, or blue.
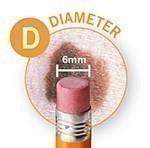 D = Diameter
D = Diameter
Melanomas are usually greater than 6mm (the size of a pencil eraser) when diagnosed, but they can be smaller.
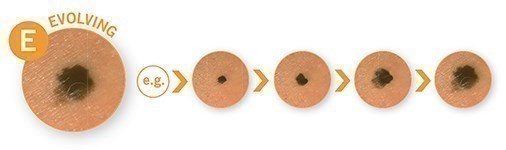 E = Evolving
E = Evolving
A mole or skin lesion that looks different from the rest or is changing in size, shape, texture or color.
Do you have a question for one of our expert providers at Dermatology Associates of Ithaca?
Call (607) 257-1107 to schedule an appointment.





